Report of Reproductive Health / Vaginal Hysterectomy Camp
at Gauri Shankar
General Hospital, Dolakha
Conducted by Kathmandu Model Hospital in Collaboration with ANMF
As Part of the Managing Genital Prolapse in Women of Rural Nepal Project

Introduction Utero-Vaginal Prolapse (UVP):
A genital prolapse or pelvic organ prolapse is a downward or forward displacement of one of the pelvic organs from its normal location in females. Traditionally, prolapse has referred to displacement of the urinary bladder, the uterus or the rectum; often accompanied by urinary, bowel, sexual, or local symptoms. Although conservative treatment is enough for mild prolapse, the primary management of severe prolapse is surgical.
Pelvic organ prolapse is a common problem in the elderly women. It is estimated that 25-35% of rural women have some degrees of genital prolapse. It is caused most commonly by pregnancy, labor, and childbirth. It also can be related to diseases that cause increased pressure in the abdomen, such as obesity, respiratory problems with a long-lasting (chronic) cough, constipation, and pelvic masses.
Conservative treatments such as pelvic floor exercises and a vaginal pessary are best in cases of mild uterine prolapse or when surgery is not an option. Surgery is the definitive treatment and can provide a long-term solution to uterine prolapse.

Introduction of Gauri Shankar General Hospital:
It is a 15 bedded hospital located at Dolakha bazaar, about 4 km from Charikot, the district headquarters of Dolakha. Dolakha is a hilly district in central Nepal. This is one of the outreach district hospitals governed and managed by Kathmandu Model Hospital / phect-NEPAL. This is run by two qualified medical doctors, nurses, paramedics and few other staff and has basic laboratory facilities, an X-ray machine, an ultrasound machine, an EKG machine, a dental chair and other basic equipment. It has an ambulance also. As an extension a clinic with laboratory and X-ray facility at Charikot bazaar is also started recently.

Reproductive Health /Vaginal Hysterectomy Camp:
The organization of the reproductive health camp was for the poor rural women of the hilly districts in and around Dolakha.
i) Background: ANMF accepted our proposal of ‘Managing Genital Prolapse in rural Nepal ‘in 2005 as a fund raising project for providing surgical treatment to 200 women with prolapse.
Charikot was chosen because of its central location so that patients from nearby hilly districts also could come and there is already a small hospital that could be upgraded by the Kathmandu Model Hospital (KMH) making it fairly well equipped for major surgery.
Preliminary discussions/planning were done at Kathmandu with members of KMH/ANMF-Nepal and also with Dr. Gaury Adhikary and others from ANMF-America at various times. There were doubts of organizing camps successfully because of deteriorating security situations and unpredictability of the waves/ foci of insurgency/counter-insurgency.
The health status of the people throughout the country has been grossly affected due to the deteriorating conflict situation and Dolakha is one of the most affected and vulnerable regions. We, the people of Nepal, are sandwiched in between the two armed forces- the state and the rebels.

ii) Steps /Activities of the camp:
- Adequate home-works /planning were done well ahead and tentative dates and place (20-29 March, 2005, Chaitra 7-16, in Dolakha) were fixed for the camp.
- Information of the free camp was disseminated through letters, telephone
calls and fax to various organizations/individuals at Dolakha districts.
Pamphlets and leaflets distribution were done. Announcement of free camp for prolapse surgery was made by Radio Nepal at prime-time just before news broadcasting time so that maximum numbers of needy women could hear and come for treatment at the camp. - Health education for prevention of prolapse was provided by distributing educational leaflets; showing documentary videos at camp and doing mothers group counseling.
- Temporary mini blood bank was established there with the help of Nepal Red Cross Society and three patients received blood transfusion.
- Additional space for postoperative care was provided by the eye hospital in its building adjoining the Gauri Shankar General hospital.
- All the surgical/medical supplies/equipments/instruments/O.R. tables' lamps were arranged by Kathmandu Model Hospital (KMH).
- Four Gynecologic surgeons and one anesthetist and two anesthetists’ assistants gave service. (Two-gynecologic surgeons from KMH, One- from T.U. Teaching hospital ( TUTH), One-from Kathmandu Medical college Teaching Hospital (KMCTH). They were there for various period of time.
- Two outpatients departments (OPD’s) were set up for patient selection,
screening for surgery, counseling and treatment of other gynecological diseases.
One was in Gauri Shankar Hospital itself and other was in Charikot bazaar proper
(about 4 km away from the hospital)
Three rooms were reorganized into operation rooms with tables/ lamps/ equipment / monitors. Up to four operation tables were run simultaneously so that we could operate on maximum number of patients. In fact, initially it was planned that only 50 cases will be operated and medical / surgical supplies were taken from Kathmandu with that estimation. But, there was overwhelming numbers of patients needing operation so extra manpower (gynecologic surgeons) and extra supplies were arranged from Kathmandu and a total of 92 operations could be made possible.
All the patients/visitors were transported to and from hospital/clinic by a vehicle of KMH. - Patients were counseled pre-operatively and informed consent was taken in all cases.
- Beds/mattresses/ SUKULS/ pre-op/ post-op medications were provided free of cost to all the patients but food was prepared/arranged by the patient themselves.
- All basic pre-operative investigations (including CBC, urinalysis, blood biochemistry, Chest X-ray, and ECG) were done free of cost.
- Patients were managed in the hospital for the first 24 hours for immediate and intensive post-operative care and then shifted to another building for routine care. As we had beds for only 20 patients in the hospital, we had to shift the patients to another building from second day onwards.
- Patients were discharged after 5 to 7 days of operation and free medications were provided at the time of discharge and asked to come for follow up after one week. Long-term follow up is being done in the Gauri Shankar Hospital.
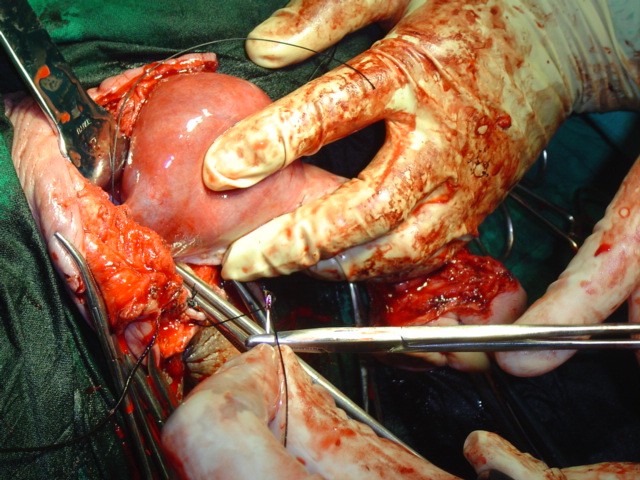
- It was historic in the sense that it was first time in Nepal where that many numbers of vaginal hysterectomies were performed in a rural health camp set up.
- A total of 45 persons were directly involved in the camp. The team comprised of medical/administrative persons. Among them 12 were doctors, 14 were nurses, 6 were paramedics (list attached).
- Ninety-two major surgeries were performed at the camp. (List attached) Patients’ age varied from 30 to 88, all were multiparous women. The patients having second degree/third degree prolapse and procedentia were selected for operation. Most of patients come from Dolakha, and other adjoining districts of Ramechhap, Okhaldhunga and Sindupalchowk. Because of the overwhelming number of patients, not all the patients could be operated. We promised to go back there before Dashain to operate on the remaining patients.
- There were no major complications in the operated patients. Few patients have minor problems. Only three patients needed blood transfusion due to significant blood loss during surgery.
- Educational program was also an integral part in the camp.

One of the major activities before, during and after the camp was to incorporate educational component in the project aiming at prevention of the prolapse and capacity building of the team of health professionals to give quality care to the patients and to make the program viable and sustainable in the future. All the health professionals were oriented before going to the district by involving them in the several presentations/ lectures at Kathmandu Model Hospital. Clinical Protocol was developed (Attached at the annex) and distributed to all the staff (Doctors, Nurses, Paramedics, etc.) beforehand. In-service practical trainings were provided to gynecologists, medical officers, nurses and paramedics at the camp.
Other educational activities included providing health education on matters related to genital prolapse to the mothers group and general public by organizing documentary shows at camp site. Educational leaflets with an emphasis on preventing prolapse were also distributed in the district.

Discussion
A free Hysterectomy and Gynaecological camp was conducted in Gauri Shankar General Hospital, Charikot, Dolakha from 7 to 16 Chaitra, 2061(20-29 March,2005). It was organized by Kathmandu Model hospital, with the financial assistance from America Nepal Medical Foundation (ANMF), America. Phect-NEPAL/ Kathmandu Model hospital did coordination and also provided human resources, equipment/instruments, medial/surgical supplies, hospital buildings, guest houses and volunteers.
Nepal Red Cross Society helped in managing the mini blood transfusion center during the camp period. Other organizations including RHDP, RHIYA (a phect-NEPAL project), and the eye hospital at Charikot helped a lot for local logistics. Special positive output in the total camp activities was due to the ongoing regular RHIYA activities- the well oriented community activists helped in counseling.
On the occasion, Gynaecologic Surgeons : Dr. Ganesh Dangal (From Kathmandu Model Hospital), Dr Padam Raj Pant ( From T.U. Teaching hospital), Dr Aruna Karki ( From Kathmandu Model Hospital) and Dr Meena Thapa ( From Kathmandu Medical College) ; Anesthesist Dr. Ajit Shrestha ( From T.U. Teaching Hospital) and other Physicians Dr. Hemab Rajbhandary , Dr. Bibta Pradhan, Dr Santosh Gurung , Dr Kamal Wagle, Dr Rup Kamal Sainju, Senior nurses Ms Shusila Shakya, Ms Radhika Ghimire, Ms Ranju Devkota and other sisters / staff gave major and memorable contribution in surgery, examination, screening , counseling and treatment of the patients. Other Health Professionals of Kathmandu Model Hospital and Gauri Shankar General Hospital helped for examination, diagnosis and treatment. Dr Bharat Pradhan (Director of Kathmandu Model Hospital and former health minister), Ms Bindu Gurung (Matron of Kathmandu Model Hospital), Mr Taranidhi Dahal and Mr Hemanta Joshi took care of the overall management in the camp.
516 different types of patients were examined, treated and counseled. They came from the entire VDCs of Dolakha district; some are from very remote parts (about 1 and half days walk) of the district and from Ramechhap, Sindhupalchowk, and Okhaldhunga districts. Out of them, 247 cases were Utero-vaginal prolapse of different degrees and it was over 50% of all gynaecological patients. The highest percentage was 2nd degree i.e. 42 and 53 of 3rd degree and 5 of first degree. Among them, vaginal hysterectomy with pelvic floor repair was performed for 90 patients and anterior and posterior cholpoperineorraphy for remaining two. In addition to hysterectomy, two patients also received surgery for repair of their rectal prolapses.
Even though, this surgical operation and the anesthetic procedure are supposed to be major ones in tertiary hospitals, there was no single unwanted and risky event in the operation theatre.
The socioeconomic condition of the patients was very poor. Some of them came from the marginal communities. It was very difficult job to select 92 UV prolapse cases among them. They spent their life in carrying heavy loads of grains, fodder, water and fertilizers. The saddest part of the story is they used to carry about 50 k.g. of load on their backs and climbed up and down 3 to 8 times a day for half an hour to 3 hours. They told their sorrowful story that they used to walk carrying 3 to 10 times of 2 Gagries (about 10 to 25 liters in 1 Gagry) to 10 Gagries of water every day when the symptoms of uterine prolapse was first seen and also they told the better part of the story is that they have safe drinking water in their home and near their home these days.
It seems that the contributing factors of the UV prolapse are early childbirth , low spacing i.e. not using family planning means, having more children ,longer labor pain and not assisted by the trained health personnel , doing heavy work immediately after child birth , low socioeconomic condition so that female has to do every work in their home and not having nutritious food and they have smoking habit and used to cook food in a kitchen that is full of smoke and developed chronic cough so it contributes to UV prolapse.
Some patients with UV prolapse who have no severe infections and ulcers were applied ring pessary inside the vaginal canal and advised to come after 3 months for follow up.
Among 269 gynaecological cases, cervicitis was on the top and then pelvic inflammatory disease, dysmenorrhoea, UTI, DUB and vaginitis. Curable diseases were treated (medications given free of cost), others were counseled and advised to come for follow up.
One of the major activities was to incorporate educational component in the project aiming at prevention of the prolapse and capacity building of the team of health professionals to give quality care to the patients and to make the program viable and sustainable in the future. This needs to be continued.
In the end, genital prolapse and reproductive tract infections are the major problems of the female population of Dolakha district so it will be useful to conduct such type of camps in the future. There are also a number of requests from all over the country to organize such type of camps in rural hilly districts but there are various constraints; mainly the lack of funds.